When Home Health Turnover Hits 79%, Pay Isn’t the Whole Story

In 2024, median annual turnover for professional caregivers in home care reached 79.2%, according to the Activated Insights Benchmarking Report.1 Hospital RN turnover, by comparison, sat at 17.6%.2
For the average home health agency, that gap is the difference between a workforce that grows and a workforce that drains. And most leadership teams are still trying to close it with the same playbook: higher wages, sign-on bonuses, faster onboarding, more aggressive recruitment funnels.
Those investments matter. They just aren’t enough.
A meaningful share of home health turnover is being driven by something agencies are less comfortable naming and less prepared to address: safety conditions in the field that clinicians experience daily and rarely report cleanly on an exit survey.
If your organization is losing one out of every three clinicians within their first year, this is the part of the retention equation worth examining.
What the Data Actually Says About Why Home Health Workers Leave
Most home health turnover analysis frames the problem as compensation, scheduling, or burnout. Those are real factors. They are also incomplete.
Recent research is making the safety connection harder to ignore.
A 2025 survey of more than 1,000 healthcare workers conducted by Verkada and The Harris Poll found that nearly 20% of healthcare workers have already considered leaving their positions because of safety concerns. Almost half said they were likely to leave within the next 12 months if those concerns weren’t addressed. Among nurses specifically, 61% reported being more concerned about workplace safety than when they started in healthcare.3
Home health is the harder version of that problem.
A 2024 Medbridge analysis of home health workforce data reported that 65% of home care workers have experienced verbal, physical, or sexual violence on the job. The same analysis explicitly tied unsafe field conditions to “increased sick days, missed patient visits, and higher turnover.”4 Researchers studying healthcare workforce retention have found the same pattern repeatedly: violence and the threat of violence are durable drivers of turnover intention, not occasional triggers.
Cheryl B. Jones, a healthcare workforce researcher cited by AHRQ, put it directly. Workplace violence is, in her words, “one of those things that can tip people over in their decision to leave a unit, leave an organization, and maybe even to leave the workforce.”5
For a home health clinician doing five or more solo visits per day in environments her organization cannot control, that tipping point is closer than most agencies realize.

Why Exit Surveys Miss It
If safety is such a significant retention driver, why doesn’t it show up cleanly in exit data? A few reasons.
First, departing clinicians often cite the most defensible reason rather than the most accurate one. “I’m leaving for a higher-paying role” is socially easier to write on an exit form than “I don’t feel safe doing my job.” The second reason is harder to say out loud, especially to a manager the clinician likes and respects.
Second, the safety-to-turnover pathway is rarely a single incident. It’s accumulation. A few uncomfortable visits. A close call no one outside the agency will ever know about. A pattern of feeling exposed that builds over months. By the time the clinician decides to leave, the safety thread is woven into every other reason on the list, not separable from it.
Third, agencies often don’t ask the question directly. Most exit surveys focus on compensation, scheduling, advancement, and management. Safety, when it’s asked about at all, is usually framed in compliance language (“Did you feel the agency followed safety protocols?”) rather than in operational reality (“Did you ever feel unsafe during a patient visit?”). The first question gets a polite yes. The second gets a different answer.
The clinicians who do tell agencies the truth on the way out are the exception. Most leave quietly, and the safety driver gets logged as something else.
What Safety-Driven Turnover Actually Costs
The financial case for closing this gap is straightforward, even if the precise per-employee numbers vary by source.
Hospital-side data from the 2026 NSI National Health Care Retention Report puts the average cost of replacing a single staff RN at $60,090.2 Home health doesn’t have a single equivalent benchmark, but agency leaders working in the sector consistently report replacement costs in the range of several thousand to several tens of thousands of dollars per clinician once recruitment, onboarding, training, lost productivity, and temporary coverage are accounted for.
For an agency with 200 clinicians and a 60% turnover rate, that’s 120 replacements per year. Even at conservative replacement-cost assumptions, the annual financial drag runs into seven figures.
The harder cost to quantify is the operational one. Constant churn means newer clinicians on routes more often, less institutional knowledge in patient relationships, more handoffs, more scheduling pressure on the clinicians who stay, and more patient satisfaction risk. Each of those secondary effects feeds back into the original problem: tired, stretched clinicians in the field are more vulnerable in the moments that matter, and feel it.
The agencies that treat clinician safety as a workforce investment rather than a compliance line item are the ones starting to break that loop.
What Closing the Safety Gap Looks Like Operationally
The infrastructure most agencies have for protecting field clinicians has not kept pace with how the work is actually done. Most workplace violence prevention plans were designed around facilities. Fixed alarms, badge access, on-site security, supervisor visibility down a hallway. None of that follows a clinician into a patient’s home.
Closing the gap requires meeting the work where it happens.
A few specific capabilities matter for home health clinicians specifically.
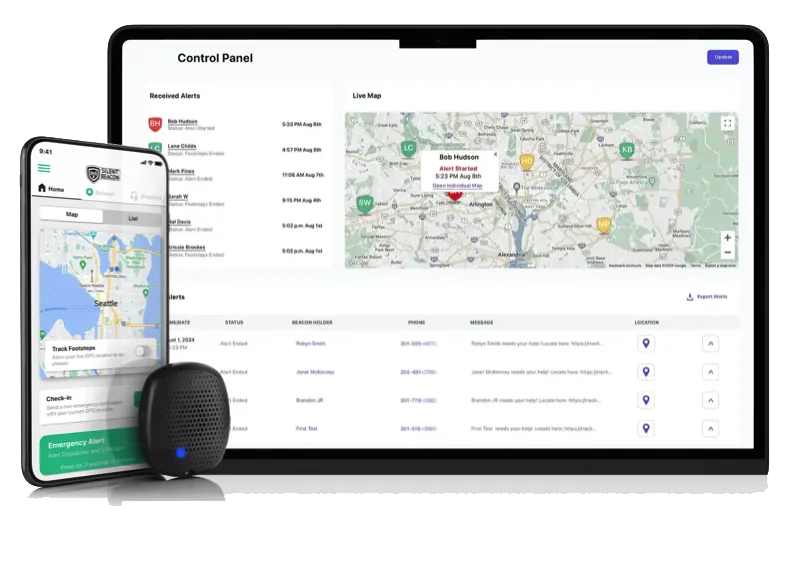
A wearable device with single-press activation removes the friction of unlocking a phone or navigating an app during an escalating situation. The clinician doesn’t have to disengage from the room to summon help. A discreet activation mode lets the clinician call for backup without alerting the person across from them, which matters in situations involving cognitive impairment, intoxication, or family-member tension.
Live route monitoring and structured check-in tools extend safety beyond the moment of crisis. A clinician walking from her car to an unfamiliar door has visibility back to her supervisor. An arrival or departure check-in replaces the inconsistent text-message protocols most agencies rely on today and creates documentation a risk team can actually use.
Live route monitoring and structured check-in tools extend safety beyond the moment of crisis. A clinician walking from her car to an unfamiliar door has visibility back to her supervisor. An arrival or departure check-in replaces the inconsistent text-message protocols most agencies rely on today and creates documentation a risk team can actually use.
These aren’t theoretical capabilities. They’re the operational expression of taking the safety-to-turnover connection seriously.
What This Means for Operations and Clinical Leadership
For COOs, VPs of Clinical Operations, and Chief Nursing Officers in home health, the question worth carrying into the next leadership meeting is sharper than “how do we reduce turnover?”
It’s: “How much of our turnover is being driven by working conditions our exit data isn’t catching, and what is the operational cost of continuing to address those conditions with tools built for buildings instead of tools built for the field?”
The agencies pulling ahead on retention right now are the ones treating safety infrastructure as a workforce investment, not a discretionary line item. They aren’t waiting for an OSHA mandate. They aren’t waiting for the next incident report. They’re closing the gap because they understand that protecting the clinicians they have is significantly cheaper, and significantly more effective, than recruiting through a 79% churn rate.
Pay matters. Scheduling matters. Career development matters. None of it replaces a clinician’s confidence that her organization has thought about her safety in the field as carefully as it has thought about her productivity.
That confidence is what shows up in retention data twelve months later.
References
- Home Care Association of America. “Home Care Turnover Rate Jumps to 80%…HCAOA is Here to Help Members!” Citing the 2024 Activated Insights Benchmarking Report (formerly Home Care Pulse). https://www.hcaoa.org/newsletters/home-care-turnover-rate-jumps-to-80hcaoa-is-here-to-help-members
- Becker’s Hospital Review. “The cost of nurse turnover in 10 points | 2026.” Summary of the 2026 NSI National Health Care Retention & RN Staffing Report. https://www.beckershospitalreview.com/workforce/the-cost-of-nurse-turnover-in-10-points-2026/
- ASIS Security Management Magazine. “Survey: Workplace Safety Concerns Influencing Turnover in U.S. Healthcare.” Reporting on Verkada and The Harris Poll, “The State of Healthcare Worker Safety,” 2025. https://www.asisonline.org/security-management-magazine/latest-news/today-in-security/2025/july/healthcare-workplace-violence/
- Medbridge. “Best Practices for Ensuring Clinician Safety in Home Health,” 2025. https://www.medbridge.com/blog/best-practices-for-ensuring-clinician-safety-in-home-health
- Agency for Healthcare Research and Quality (AHRQ) PSNet. “Addressing Workplace Violence and Creating a Safer Workplace.” Perspective featuring Cheryl B. Jones, PhD, RN, FAAN. https://psnet.ahrq.gov/perspective/addressing-workplace-violence-and-creating-safer-workplace
Talk to a safety expert about protecting your home health workforce.