What Behavioral Health Clinicians Need That Mental Health Awareness Month Rarely Talks About
May is Mental Health Awareness Month. By the end of it, most behavioral health organizations will have circulated stigma-reduction graphics, run patient awareness campaigns, and reminded the public that mental illness is a medical condition deserving of dignity and care.
All of that matters. None of it is the conversation that protects the people doing the work.
The clinicians de-escalating active psychosis in a stranger’s living room, the crisis responders sitting across from someone in suicidal ideation, the case managers walking into a substance-induced situation they cannot predict: these are the workers most exposed to behavioral health emergencies. They are also the workers least visible during the month dedicated to mental health.
This piece is for the operations and clinical leaders who are responsible for those workers. It is about what a behavioral emergency actually looks like from the clinician’s side of the room, why traditional violence prevention frameworks were not built for this work, and what protecting a mobile behavioral health workforce actually requires.
The Risk Profile Most Awareness Campaigns Miss
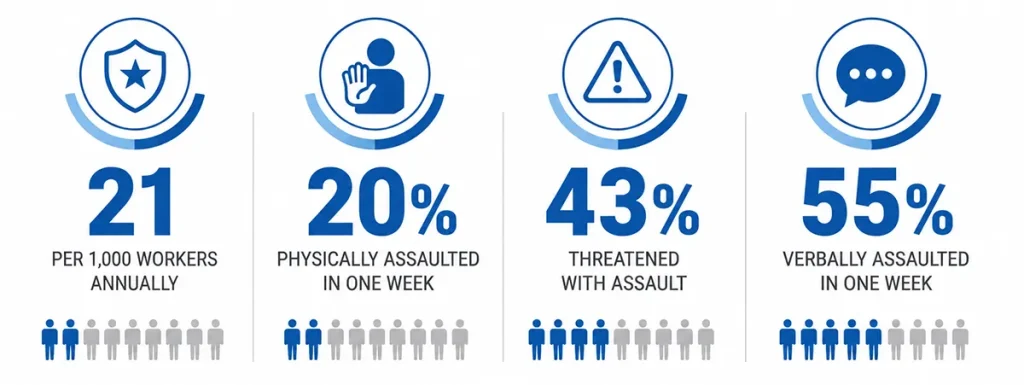
The U.S. Department of Justice reports that mental health occupations have one of the highest rates of workplace violence of any profession in the country, at roughly 21 violent crimes per 1,000 workers per year (the second-highest rate across all occupations tracked). For context, that is more than three times the rate for the workforce overall.
The inpatient data is even more direct. A widely cited study found that 20% of psychiatric nurses were physically assaulted, 43% were threatened with physical assault, and 55% were verbally assaulted in the equivalent of a single work week.
- Mobile crisis teams responding to 911 diversions and police co-response calls in private homes, vehicles, and public spaces
- Outpatient clinicians conducting community-based assessments in environments the organization does not control
- Residential staff managing behavioral escalations with no security personnel on site
- Case managers and peer support specialists working alone with clients whose stability shifts day to day
- Intake and assessment teams meeting clients for the first time with limited history
Why Traditional Violence Prevention Models Fall Short for Behavioral Health
- Fixed panic buttons protect rooms, not people. They cannot follow a clinician into a client’s home.
- On-site security cannot intervene in a crisis that happens forty minutes away in someone’s living room.
- Buddy systems and check-in protocols document risk after the fact. They do not summon help during the seconds that actually matter.
- Cell phones are the most common fallback, but they require the clinician to disengage from the situation, unlock a screen, and navigate to a contact or app while the situation is still active.
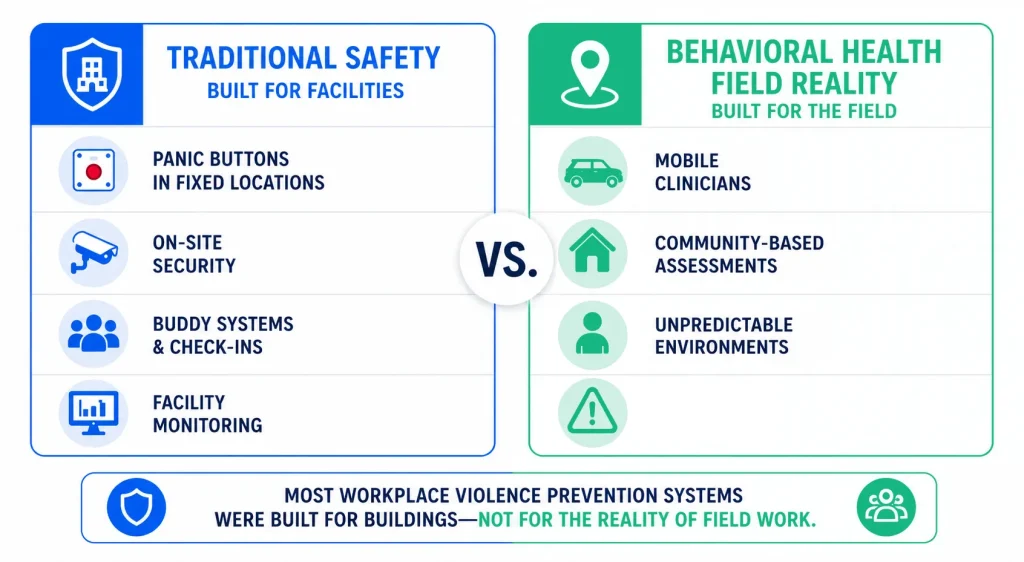
The shared problem is friction. Every second a clinician spends interacting with technology is a second they are not de-escalating, not creating distance, not reading the room. In a behavioral crisis, those seconds are the entire margin.
What a Behavioral Emergency Actually Demands From Safety Technology
If safety technology is going to function during a behavioral health emergency rather than after one, it has to meet the work where it actually happens. That means a few specific design requirements that most consumer or facility-based tools were never built to handle.
Activation has to be invisible to the person in crisis
A clinician who is de-escalating someone with paranoid ideation cannot pull out a phone. A case manager sitting across from a client experiencing a substance-induced episode cannot announce that they are calling for help. The act of summoning support cannot itself escalate the situation.
This is what a silent, single-press wearable activation is designed for. A discreet press, no screen interaction, no audible cue: help is on the way and the person across from the clinician has no idea anything has changed.
Help has to reach the right people simultaneously
In a behavioral emergency, the response is rarely just one call. The supervisor needs to know. The clinical lead needs to know. In the most acute situations, 911 needs to be on the line. A safety platform that only routes alerts internally, or only routes them to a single channel, leaves clinicians with a binary choice in a moment that demands parallel action.
Multi-channel alerting handles that simultaneously. Voice, text, email, and push notifications go out at once to the people who need to respond, while the clinician's GPS location is shared so the response is informed rather than improvised. For organizations operating mobile crisis teams or community-based programs, the ability to call 911 directly from the device, without phone interaction, closes the most dangerous gap in a crisis response chain.
Mobile crisis teams need to see each other
Crisis response is rarely done solo by design. Two-person teams, co-response models, and outreach pairs are increasingly the standard for the highest-risk encounters. But once those teams are deployed, the partner who is not in the immediate interaction often has the least visibility into what is happening.
Beacon-to-Beacon alerts, a patented two-way alerting capability, address that gap. Team members can send and receive audio and visual confirmations between their devices in real time. If one clinician needs backup, their partner knows immediately and is not relying on a yelled phrase or a missed text. For mobile crisis teams, that lateral awareness is often the difference between a controlled escalation and a dangerous one.
Field clinicians need protection during the parts of the visit no one sees
The behavioral emergency itself is one moment in a much longer day. Clinicians are also walking into unfamiliar neighborhoods, sitting in cars before visits to review notes, walking from a parking spot to an unfamiliar door, and leaving residences after difficult interactions. The risk does not end when the visit does.
Footsteps Mode shares live location with designated contacts during a route, giving clinical supervisors and operations leaders real-time awareness of where their team is when they are most exposed. Check-In Mode lets a clinician confirm safe arrival or safe departure with a custom message, replacing inconsistent text-message protocols with structured documentation. Together, they extend safety beyond the moment of crisis into the entire arc of the visit.
What This Looks Like at the Leadership Level
For Chief Clinical Officers, VPs of Behavioral Health, and Executive Directors, the practical question is not whether to deploy safety technology. It is whether the technology you have actually matches the work your clinicians do.
A few questions that surface the gap quickly:
- If a clinician needed help right now, in the middle of a community-based assessment, how would they signal it?
- How long would it take from the moment they decide they need help to the moment a supervisor or 911 dispatcher knows?
- How many steps require interacting with a phone, navigating an app, or speaking aloud?
- How much of your current safety infrastructure assumes the clinician is inside a building you control?
If those answers expose more friction than your clinical leadership is comfortable with, the gap is operational, not theoretical.
There is also a workforce dimension that often goes unspoken. Behavioral health turnover is a documented crisis, and unsafe field conditions are consistently among the leading reasons clinicians leave the profession. The organizations that will retain experienced crisis responders, mobile clinicians, and community-based staff over the next five years are the ones treating field safety as a structural investment rather than a discretionary line item.
A Different Kind of Awareness
Mental Health Awareness Month is, at its best, a public commitment to take this work seriously. The clinicians who do the work, the people who walk into the unknown to help someone in crisis, deserve to be part of that commitment.
Recognition is not protection. A campaign is not a safety plan. The behavioral health workforce needs leadership that treats clinician safety as part of the same mission that drove them into the field in the first place.
Awareness is the easy part. Building the infrastructure that protects the people delivering the care is the work.
Talk to a safety expert about protecting your mobile behavioral health workforce.